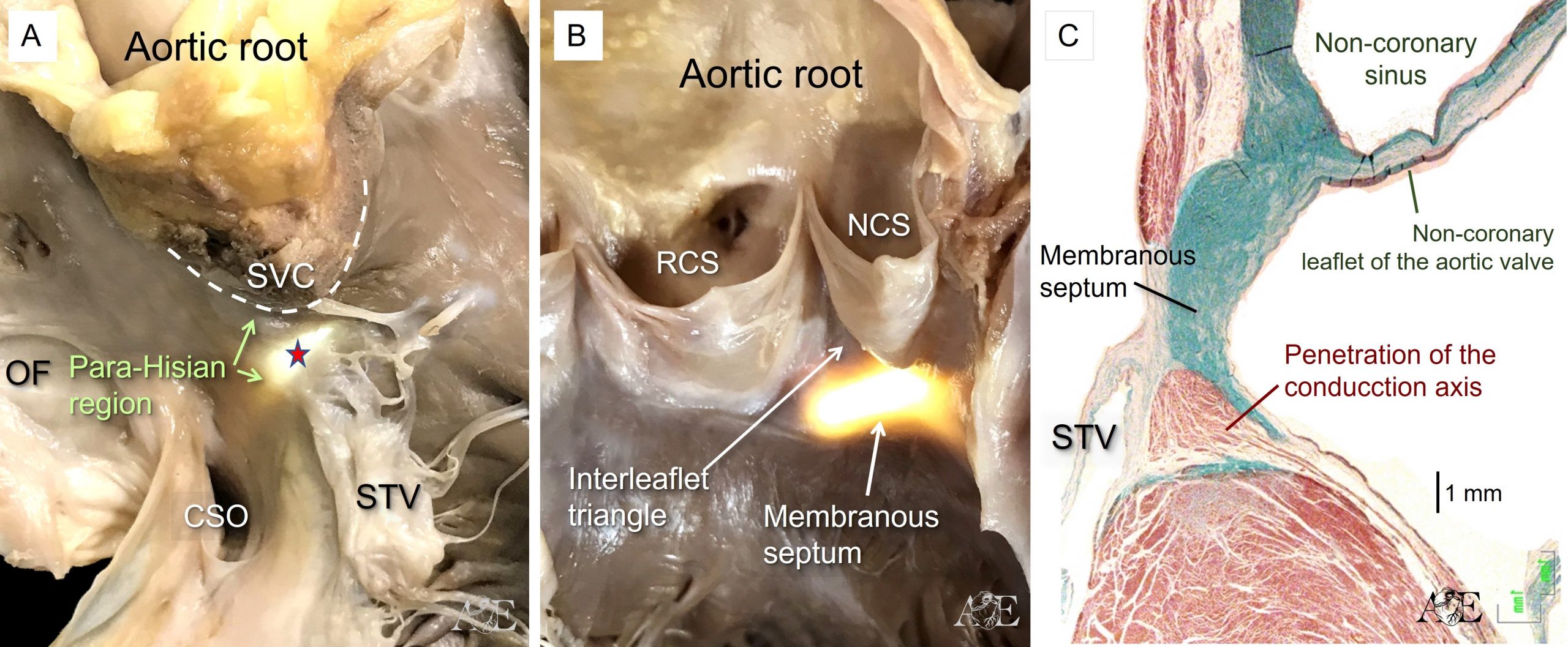
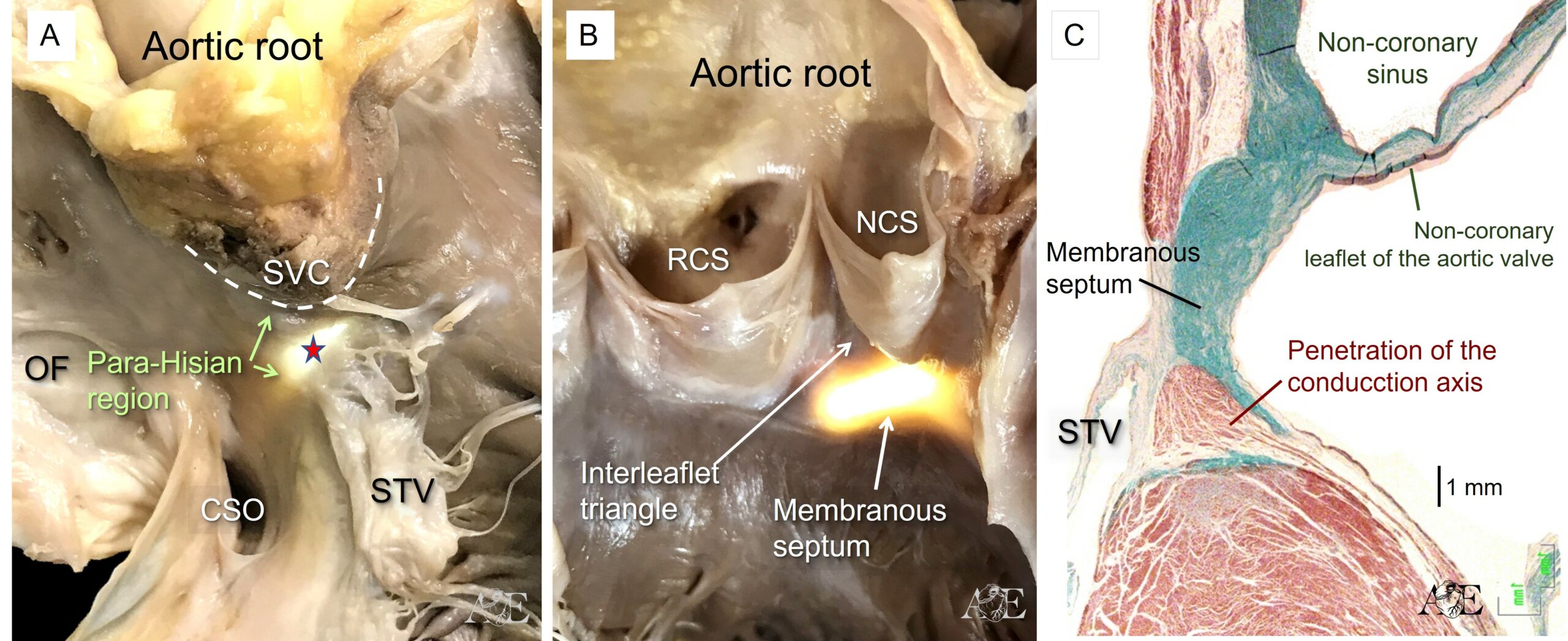
Sections taken cranially, cutting through the non-coronary aortic sinus, show the relationship between the hinge of the non-coronary leaflet of the aortic valve and the basal extent of the left bundle branch (Figure 4c). This histological section also shows the fibrous membranous septum that is the truly atrioventricular septal structure.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}