ICE Cases
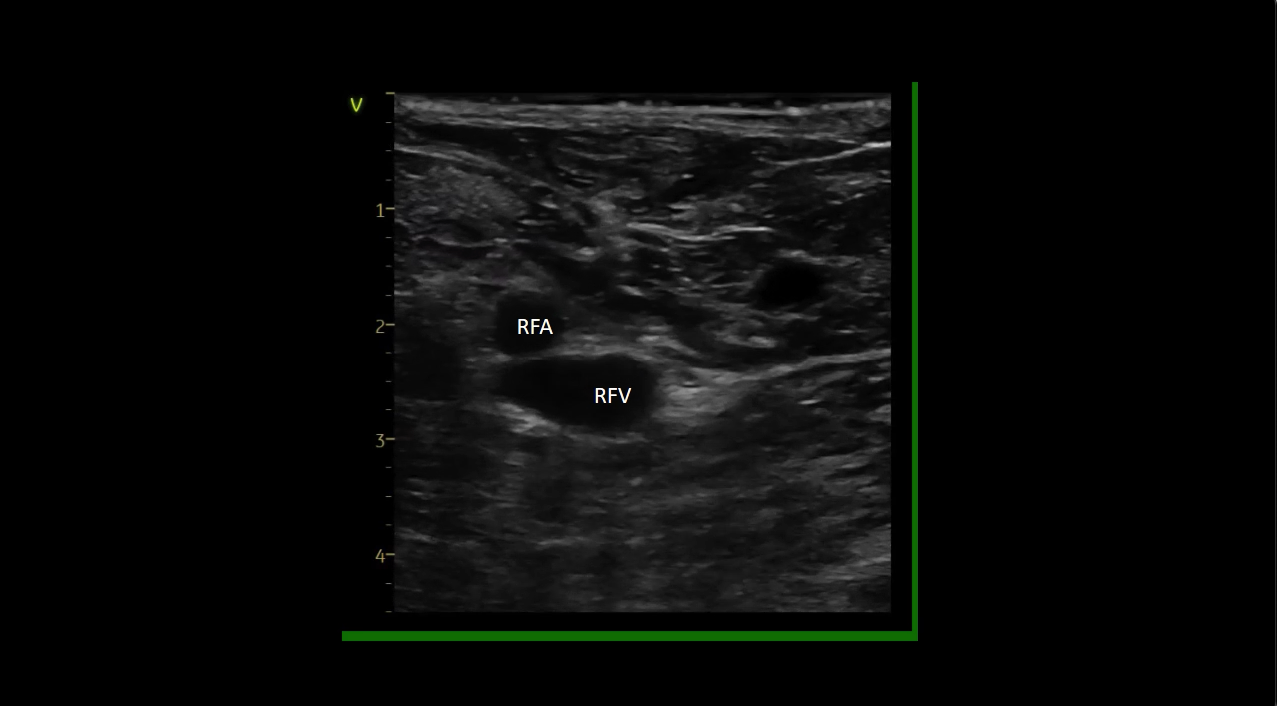


Video 1. Short axis view of iliofemoral vessels using ultrasound. Right femoral artery (RFA) is seen more lateral and superior. Needle is observed tenting the anterior wall of the right femoral vein (RFV) before entering. Guidewires are seen advancing into the RFV.
Video 2. ICE guided contours are drawn as a first step to define LA structures to guide TS access and LA mapping.
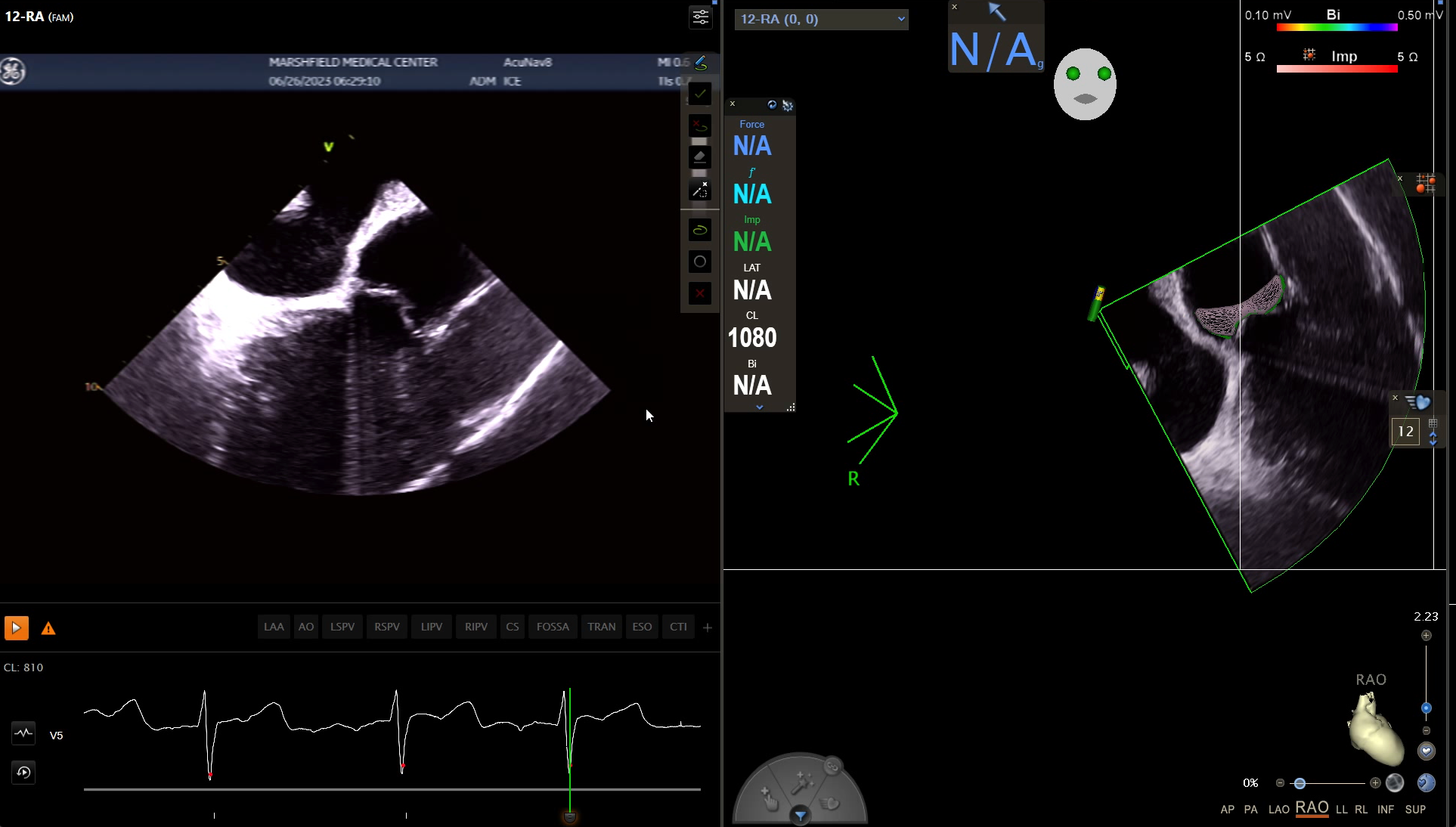
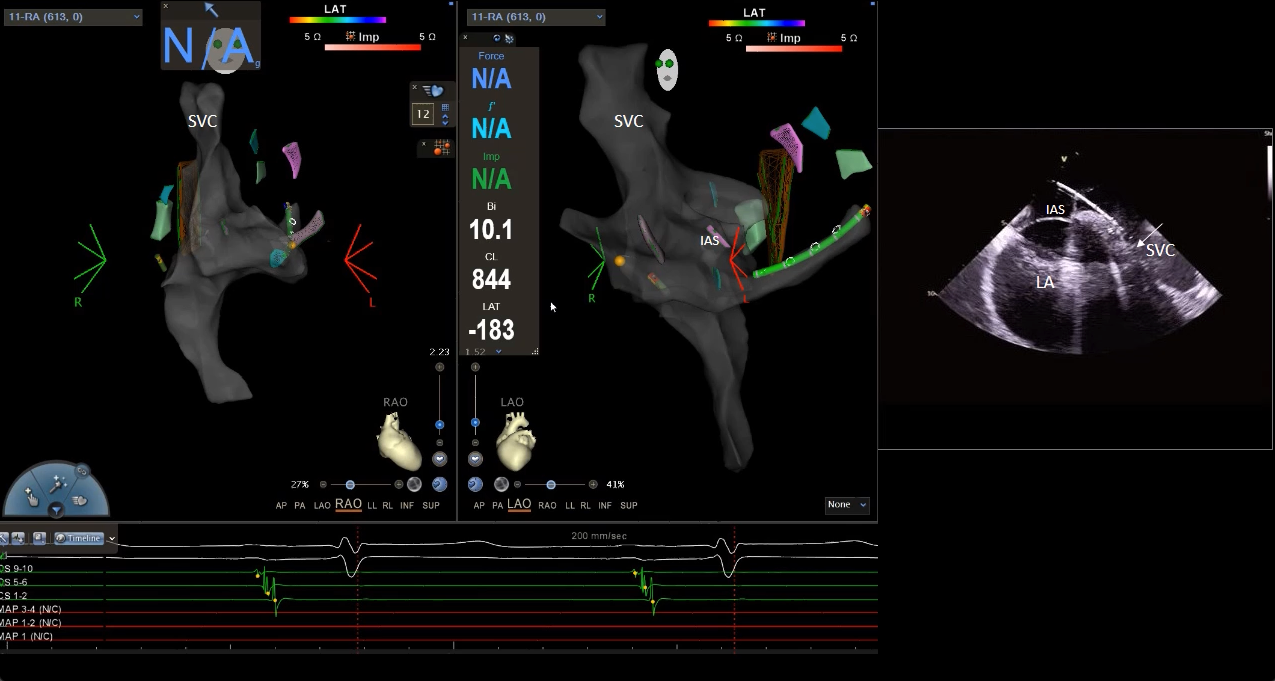
Video 3. Left panel. Advancement of Vizigo sheath (Biosense Webster) from the inferior vena cava into the right atrium and superior vena cava in preparation for transseptal access. RAO and LAO projections of the RA fast anatomical map (FAM) with CartoSound based geometry of left atrial structures as seen on figure 1 and video 2. Right panel: Still ICE frame of RA long axis view showing the position of the TS sheath in the SVC/RA junction.
Video 4. Transseptal access. 3DEAM in orthogonal views and ICE FOV on the IAS shows tenting before crossing with the TS needle and saline bubbles seen in the LA. Forward pressure on the TS sheath as the dilator is pulled back allowed for crossing of the sheath.
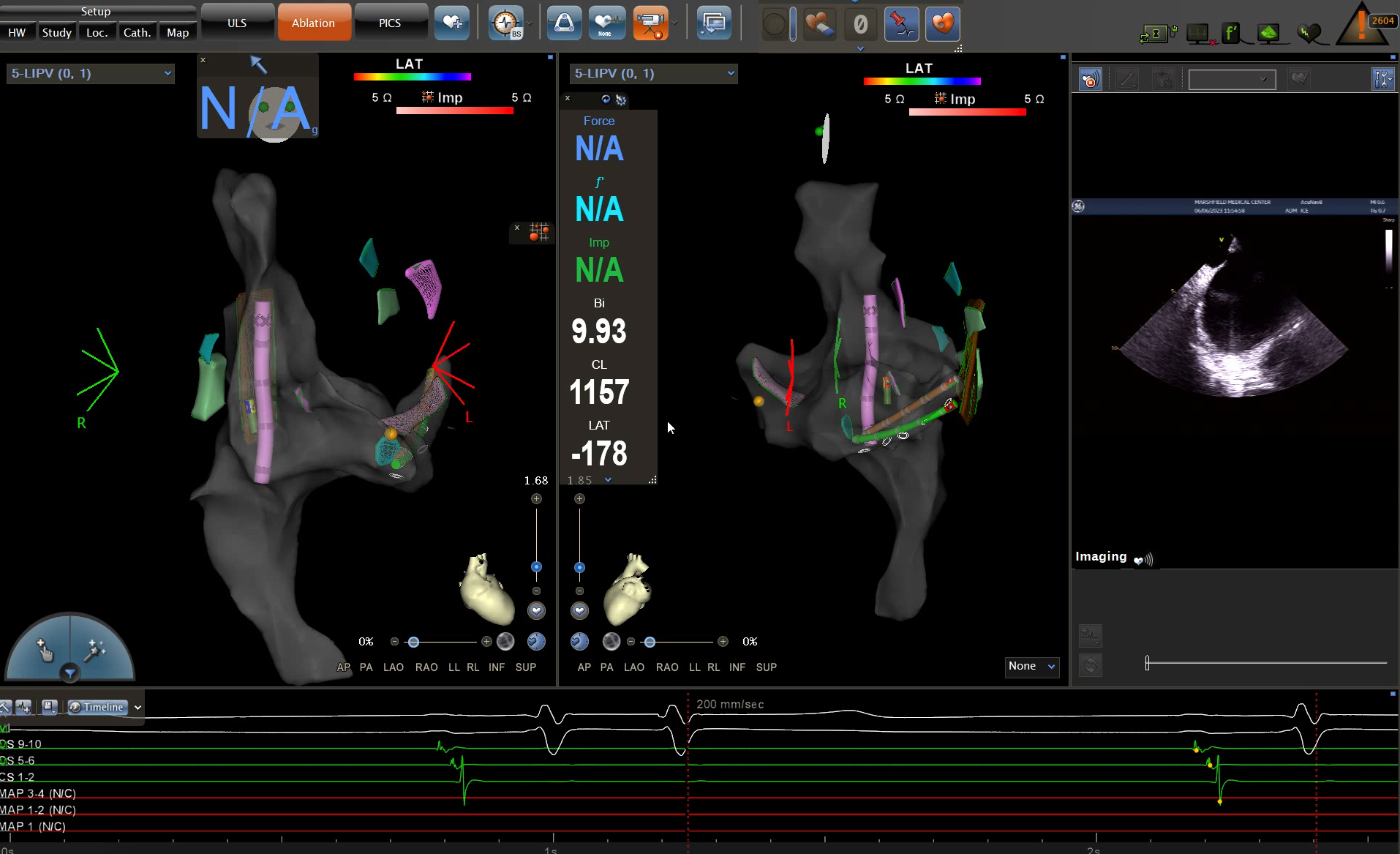
Video 5. Transseptal access using a J guidewire for sheath advancement. The TS sheath did not cross with forward pressure. The TS needle was removed and a J guidewire was placed inside the LSPV and the TS sheath and dilator were advanced. During crossing the tenting disappears on ICE and the TS sheath is seen advancing towards the LSPV on 3DEAM. LA sheath placement is confirmed on ICE by readjusting the FOV after crossing.
Video 6. Fast anatomical map (FAM) of the LA (patient in AF) at 4X speed. Observe the synchronous movements between the TS sheath and the multielectrode catheter during mapping.
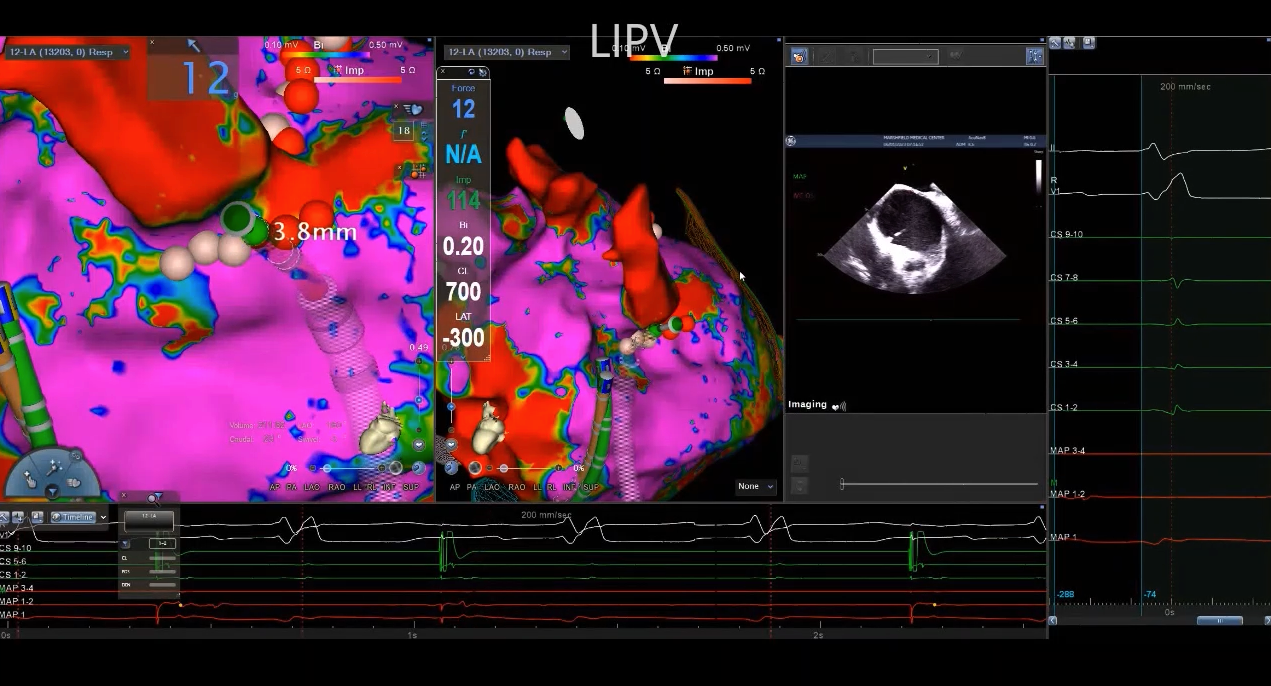
Video 7. ICE and 3DEAM guided ablation. Sequence of ablation presented is LIPV, LAA ridge, posterior wall near the RSPV and RIPV. A stability protocol including low tidal volume and CS pacing was used to minimize catheter movement. Catheter contact is confirmed with ICE views and force vector.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}